Surgery and Anatomy in the Ancient World
The Prehistoric World
Surgery ‐ was limited by their knowledge of the human body and the tools they had available, however there is evidence that their procedures were successful:
They would cut a hole in the skull in order to let out bad spirits which were believed to be the cause of severe headaches. This is called trephining (sometimes trepanning). Many patients survived this operation, which is shown by skulls which show evidence that the wound started to heal.

{kind=link}
A healed trepanation wound
There is evidence that prehistoric people may have used splints in order to stabilise broken bones to allow them to heal naturally.
Recent evidence has suggested that some prehistoric people were able to perform amputations which the patient also survived. This suggests that they were able to controlbleeding and infection to some degree.
Anatomy – their knowledge of the human body was limited. Some basic knowledge is indicated by:
Cave paintings show animals being speared through the heart which shows an understandingthat the heart is an important organ.
Attacks by wild beasts would have caused some serious injuries to people, allowing some knowledge of the inside if the body to be gained.
Ancient Egypt
Surgery – Ancient Egyptian surgery improved on prehistoric surgery for a few reasons:
Egyptian metal working was better so that surgeons had sharper and stronger tools to work with. They could perform more minor surgery e.g. removing tumours.
Egyptians understood that honey had healing properties and it was used to treat wounds.
They bandaged wounds and kept them clean.
Anatomy – Ancient Egyptian understanding of the human body also improved on prehistoric times:
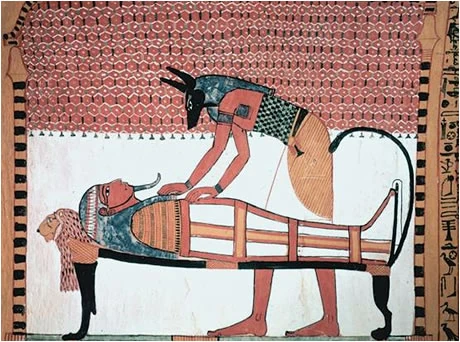
The process of mummification involved the removal of the internal organs of the body in order to preserve the body for the after‐life. This gave them a better understanding of the inside of the body. The Egyptians had names for the heart, lungs, liver etc.
{kind=link}
Mummification
The Egyptians believed the heart was the centre of the body where the soul of a person wasto be found and thinking took place. They thought that the heart was connected to the rest of the body through channels.
The Egyptians wrote down their knowledge on papyrus scrolls which allowed future generations to build upon it.
However, there were limitations to Egyptians’ knowledge:
‐ Embalmers (who did the mummification) were not doctors and would not have passed on much knowledge about the internal organs.
‐ The internal organs were also preserved in separate jars, so they were not dissected.
‐ Human dissections were not allowed because the whole body was needed for the after‐life.
Ancient Greece
Surgery – Greek surgery improved on the Egyptians:
The Greeks used wine and vinegar to clean wounds. These would have acted as antiseptics.
Greek metal was even stronger and sharper than Egyptian allowing more precise surgery.
Greek surgeons even successfully operated to drain the lungs of a patient suffering from pneumonia.
The Greeks fought many wars and surgery dealing with war wounds improved with this experience, e.g. removing arrowheads, setting broken bones.

{kind=link}
Greek surgical tools
Anatomy – This was the biggest area of improvement in Ancient Greece:
Aristotle carried out many animal dissections and argued that all knowledge should be based on careful observation.
The city of Alexandria was founded by Alexander the Great in 331 BC. It became the centre of learning based around the university and enormous library. Alexandria was the only place in the Ancient World where human dissections were allowed.
The greatest Greek doctor working in Alexandria was Herophilus. He discovered:
‐ it is the brain which controls the body
‐ the difference between arteries and nerves
‐ the different parts of the stomach and intestines
‐ the link between the beat of the heart and the pulse
Ancient Rome
Surgery – the Romans continued the successful progress of the Greeks:
They used opium as a mild anaesthetic.
The Roman Army developed more and more techniques to deal with injuries suffered in battle. Each major Roman Army camp had a sophisticated hospital.
Anatomy –
Galen (who was born in Greece) trained at Alexandria. He travelled to Rome and became doctor to the Roman Emperor. Galen performed live dissections of animals to demonstrate his knowledge of anatomy. Most famously he cut the spinal cord of a pig at different places to show that the nerves control different actions in the body.

{kind=link}
Galen wrote many books about anatomy. These were largely based on his dissections of animals. The books contained a lot of useful knowledge but also had some errors as the human body is not the same as other animals.
(ii) Surgery and Anatomy from the Middle Ages to the Renaissance
The Middle Ages
After the fall of the Roman Empire, there was a period of decline in knowledge and understanding of surgery and anatomy during the Dark Ages. After this, the Middle Ages saw a recovery of knowledge.
By the end of the period (about 1450 AD) the standard of surgery and anatomy was probably back to Roman levels.
Surgery – surgeons were looked down on by other doctors in the Middle Ages. Surgery was not thought to be a proper part of medicine. Most surgeons were barber‐surgeons who learned their trade as apprentices not at university.
Compared to the Dark Ages, there was significant improvement in surgery during the Middle Ages:
The large number of wars in the Middle Ages gave surgeons plenty of opportunity to practise operations. Pictures of ‘Wound Men’ show all of the injuries that surgeons learnt to deal with.
John of Arderne was the most famous medieval surgeon in England. He developed new methods based on careful observation and practice.
Surgeons in the Middle Ages made mild anaesthetics using hemlock and henbane
However, surgery in the Middle Ages was still limited in development because:
{kind=link}
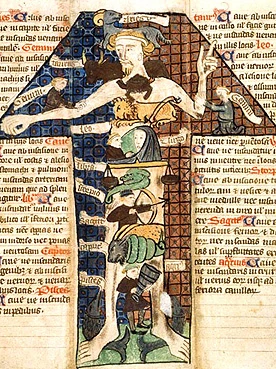
A Zodiac chart used by Medieval physicians
Surgeons still relied on supernatural beliefs such as consulting a Zodiac chart to work out the best time to operate on a patient.
Anatomy – unlike surgery, anatomy was considered to be a proper part of medical training and was studied at the universities where doctors trained. Like surgery, knowledge of anatomy began to improve in the Middle Ages after the decline of the Dark Ages:
At first dissections were banned by the Church which ran all of the universities where anatomy was studied. This was because the body would be needed in the after‐life. Later in the Middle Ages, the Church allowed each university to do one dissection per year on a convicted criminal’s body. These dissections were carried out by an assistant whilst the professor would read out from Galen’s books. If there was a difference between the body and the book, they thought that the body must be wrong. Despite these limitations, these dissections did improve people’s knowledge of anatomy.
The Renaissance
Surgery – most surgery in the Renaissance stayed much the same as in the Middle Ages. Surgeons mostly only performed three operations – trephining, amputations and removing tumours.
{kind=link}
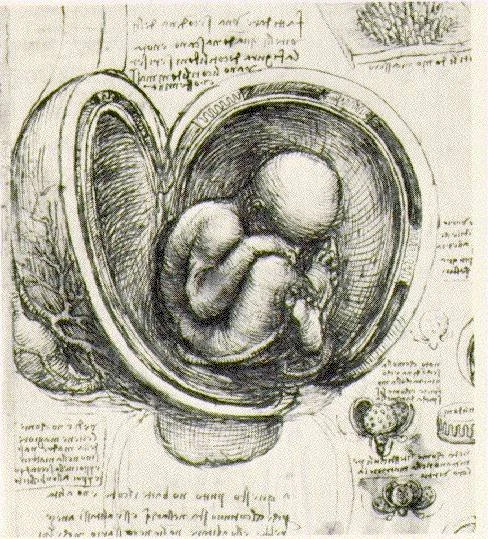
Leonardo da Vinci's detailed illustrations of the human body helped anatomy
One surgeon who did make advances during the Renaissance was Ambroise Paré:
After working as a barber‐surgeon, Paré got a job as a surgeon for the French Army. The traditional method of treating gunshot wounds was to pour boiling oil into the wound to cauterise it (burn it). This was agonisingly painful. Paré ran out of boiling oil during one battle when there were lots of French casualties – he was forced to improvise. He came up with a new ointment using turpentine, which he had read about in a book about Roman surgery.
The new ointment worked very well and he never used boiling oil again.
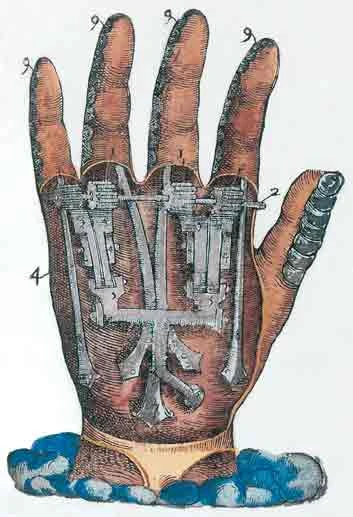

{kind=link}
Pare's design for a prosthetic hand
Paré also used ligatures (made of silk thread) to tie the ends of arteries after he had done an amputation. This was instead of the traditional method of cauterising the stump with a hot iron bar. Again, this was better because the patient did not suffer agonising pain. The one drawback with Paré’s ligatures was that he did not know they had to be sterilised, so the wounds often got infected and many surgeons stuck to the old cauterising method.
Anatomy ‐ there were certain features of the Renaissance which allowed advances to be made in the knowledge of anatomy:
Reduction in the power of the Church – this meant that universities were not limited to one dissection per year any more. It also encouraged doctors to challenge the work of Galen, who the Church had believed was right about everything.
Scientific study – there was much more interest in the Renaissance about finding out things through observation and experiment rather than just relying on books.
New artistic techniques – much more accurate pictures could be drawn of the human body which allowed doctors to learn more and share their knowledge.
The printing press – books could now be mass‐produced so doctors could circulate their new knowledge much more widely and quickly.
Two doctors in the Renaissance who made hugely important breakthroughs were
Andreas Vesalius and William Harvey.
Andreas Vesalius became Professor of Anatomy at Padua University in Italy in 1537. He contributed a huge amount to the understanding of anatomy in the Renaissance because:
He studied the human body itself and did not just rely on Galen’s books. Vesalius is said to have stolen the body of an executed criminal when he was a student in order to study the skeleton. He performed many public dissections at the university.
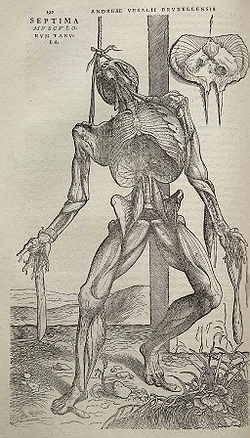

{kind=link}
An illustration from Vesalius' Fabric of the Human Body
He pointed out several mistakes which Galen had made including:
‐ the human jaw is only one bone not two as Galen had said
‐ the septum in the middle of the heart does not have tiny holes in it as Galen had claimed
He wrote a book on anatomy called On the Fabric of the Human Body, which was read across Europe. The book contained many accurate pictures of the human body.
William Harvey proved that the heart is a pump and that the blood circulates around the body.
Harvey is typical of the Renaissance because:
He challenged Galen’s ideas about the heart and the nature of veins and arteries.
He proved his ideas through careful experimentation, observation and measurements. For example, he dissected live lizards to observe their hearts beating. He tried to force thin rods and liquids the wrong way up arteries to show th
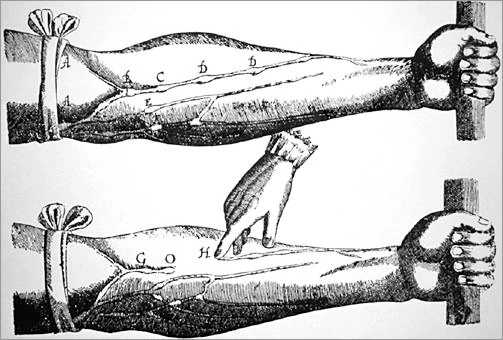
{kind=link}
One of William Harvey's experiments, showing that blood only flows one way
at the blood circulated in one direction.
He wrote a book about his discoveries.
He faced opposition from other doctors who were unwilling to believe that Galen could be wrong.
Conclusion
Both Vesalius and Harvey made very important discoveries about anatomy which laid the foundation
for future advances. However, during the Renaissance their ideas did not contribute much to improving treatments or surgery. For example, William Harvey continued to use bleeding as a treatment even though he had proved that there is the same amount of blood in the body at all times.
Ambroise Paré did improve the treatment of gunshot wounds but this would only have affected a small number of people.
(iii) Surgery and Anatomy since 1800
The Nineteenth Century
In 1800, surgery was still very dangerous. The death rate during and after surgery was still very high – around 50% ‐ for three main reasons: PAIN, INFECTION and BLOOD LOSS. Over the next century (plus a little bit) these three problems were reduced and surgery became much safer.
Pain
Many patients died of shock due to the pain of surgery. In the 1840s surgeons became interested in chemicals which could relieve pain, i.e. anaesthetics. The first of these was nitrous oxide (laughing gas) which was especially used by dentists. It was not ideal though because it could not knock out patients sufficiently for major operations. The second chemical tried was ether. This was more powerful but it has some drawbacks – it irritated the patients’ lungs; it made patients vomit; and it was mildly explosive.
In 1847, James Simpson decided to try to find a more suitable anaesthetic. He sniffed a range of chemicals until he found chloroform. This was powerful enough to knock out patients without the side effects of ether. He first used small doses to ease the pain of women giving birth. Simpson faced a lot of opposition, for example:
‐ Some religious leaders thought that it was unnatural and against God’s wishes for the pain of childbirth to be reduced.
‐ Some doctors were concerned that it was difficult to decide on the correct dose (this was made worse when one patient died of too much chloroform in 1848.
‐ Other doctors claimed that chloroform might have long‐term side effects which were not yet known.
Simpson argued back against all of these objections and he was greatly helped when Queen Victoria used chloroform to help with the birth of her eighth child in 1


{kind=link}
An inhaler for chloroform
857. After this, chloroform became widely used for all types of surgery.
Anaesthetics were hugely successful in overcoming pain in surgery, however, they actually made the problem of infection worse. This was because surgeonscould now take longer over operations as the patient was not writhing around in agony and they could also cut more deeply into the body. Both of these developments meant that more germs could get into the body.
Infection
In 1864, Joseph Lister read Louis Pasteur’s work on Germ Theory and became convinced that germs were the cause of ‘hospital fever’ (the name for the infection which many patients died of after surgery). Lister decided to look for something which would kill the germs in his operating theatre. He developed carbolic acid as the first antiseptic.
He tried it out on a boy called James Greenlees who had badly broken his leg. Normally the leg would have been amputated, but Lister set the leg straight and wrapped it in bandages soaked with carbolic acid. The boy’s leg healed perfectly and he suffered no infection. Lister then developed a carbolic acid spray to disinfect the area around an operation. Later, he soaked all of his tools in the acid too. The death rate for Lister’s operations fell from 50% to 15% in just 4 years.


{kind=link}
Like Simpson, Lister also faced a lot of opposition, for example:
‐ Many surgeons still did not believe in Germ Theory. They could not accept that something as small as a germ could kill a human.
‐ Lister was not a good public speaker. His speeches were quite boring and his written notes were very detailed and hard to read.
‐ Lister kept changing his methods to improve them, but some surgeons said this was because they were no good.
‐ Carbolic acid irritated surgeons’ hands and skin.
‐ Operations with carbolic acid became slower and more expensive which put a lot of surgeons off.
Lister slowly overcame this opposition when he showed that the death rate in his operations had fallen as low as 5%. He was also helped by the work of Robert Koch who discovered the specific bacteria which causes septicaemia in 1878. Lister could then demonstrate that his carbolic acid could kill the germ which caused blood poisoning.
Aseptic Surgery was an improvement on Lister’s antiseptic surgery. In the 1880s and 1890s, surgeons developed new techniques which aimed to prevent germs getting into the area of the operation at all.
These new ideas included:
Sterilising surgical instruments with steam. In the 1880s, Robert Koch demonstrated that steam was more effective than carbolic acid at sterilising the tools.
William Halsted, an American surgeon, invented sterilised rubber gloves in the 1890s.
Operating theatres and hospitals were rigorously cleaned.
As a result of these improvements new types of surgery could be attempted. The first successful operation to remove an appendix happened in the 1880s and in 1896 the first operation to repair a heart was carried out.
The Impact of the First World War
Blood Loss
Surgeons had tried blood transfusions for many years to try to overcome the problem of excessive bleeding during surgery. However, they could not work out why many patients died after receiving blood from someone else. In 1901, a German doctor (Landsteiner) discovered that there were different blood groups and that you could only give certain types of blood to different patients.
After this discovery successful blood transfusions could take place, but there was one major limitation - the person giving blood and the patient receiving it had to be lying next to each other because if they tried to store the blood it would simply start to clot.
During the First World War (1914'‐'18) the need for a better method of blood transfusion became urgent. There were thousands of wounded soldiers whose lives could be saved if a way of storing blood could be discovered. During the war scientists worked together and actually developed two ways of storing blood:
They found that if you separate the blood cells from the liquid part of blood (plasma), the cells could be stored in ice. When they were needed, the blood cells could be rehydrated with saline solution.
Other doctors discovered that by adding sodium citrate to blood it stopped it from clotting
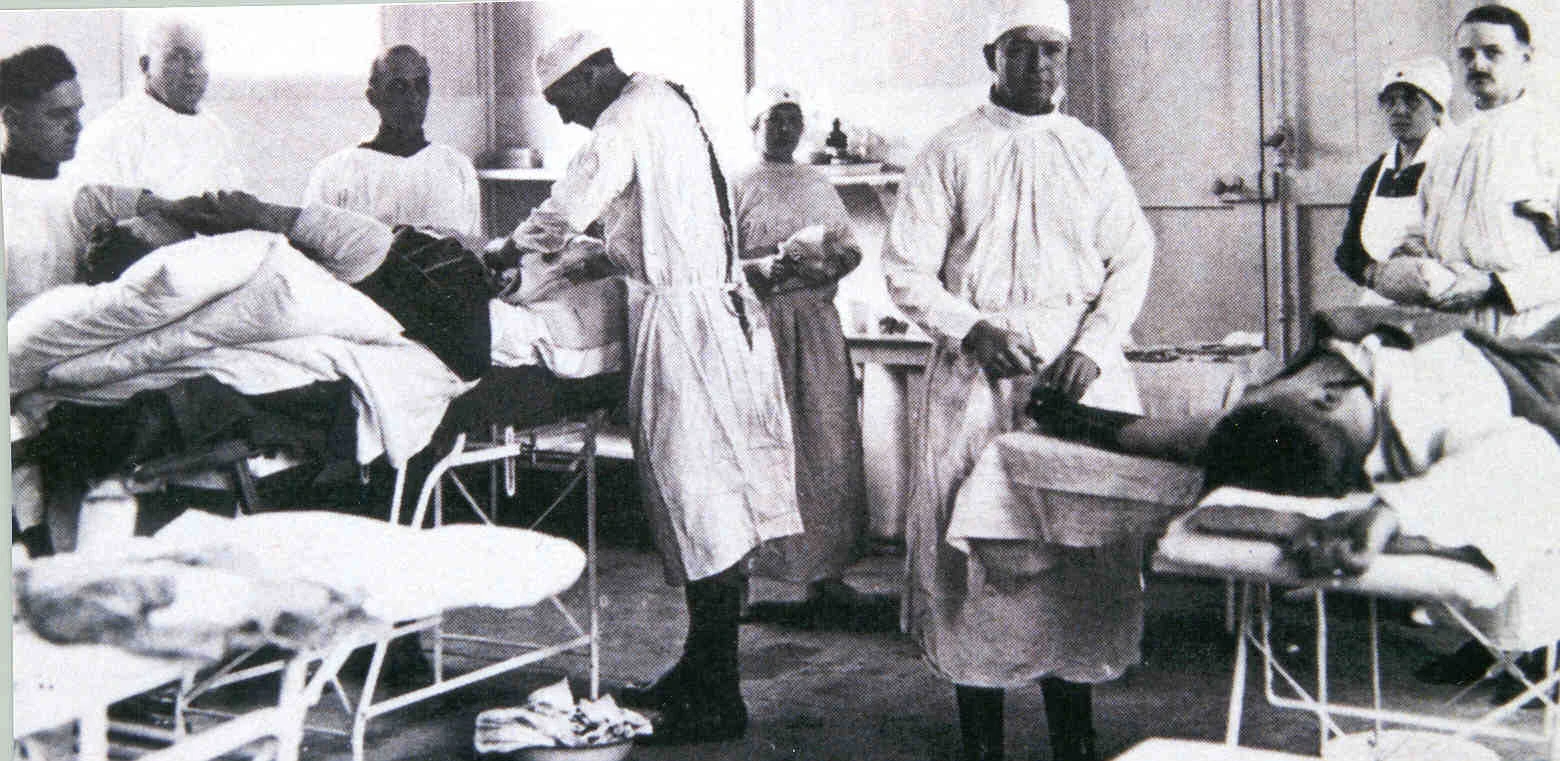
{kind=link}
WWI Field Hospital
Conclusion
Between 1840 and 1918, therefore, the three main causes of death during and after operations (pain, infection and blood loss) had been massively reduced. However, surgery in 1918 was still more dangerous than it is in the present day because, throughout the rest of the 20th century and up to the present day, scientists and surgeons have continued to make important breakthroughs in the technology and safety of surgery.
X‐Rays
X‐rays had first been discovered by a German scientist – William Röntgen – in 1895. He discovered that the rays could pass through human flesh but not bone or metal. X‐ray machines were immediately developed and installed in hospitals.
The First World War had a significant impact on the development of x‐ray technology because of the number of wounded soldiers who needed to have bullets or shrapnel removed from their bodies. X‐rays proved very useful in allowing surgeons to accurately locate the metal objects inside the body. During the war the first mobile x‐ray machines were invented.

{kind=link}
WW1 portable X-RAY vehicle
The Twentieth Century
The speed of advances in surgery increased dramatically in the 20th century, for example:
Plastic Surgery
The solution to the problem of storing blood for blood transfusions happened during the First World War (1914‐18) which was in the 20th century. Another advance which was speeded up by the First World War was the development of plastic surgery. Harold Gillies set up the first dedicated centre for plastic surgery in England in 1917. Gillies’ cousin – Archibald McIndoe – continued his work in the 1930s. In 1938, McIndoe was appointed as Consultant in Plastic Surgery to the R.A.F.
During the Second World War (1939'‐'45), Archibald McIndoe operated on many badly burned aircrew. He reconstructed their faces but also recognised that they would need psychological support in order to recover. He called the airmen his ‘Guinea Pigs’ and the Guinea Pig Club still meets today to honour him.
{kind=link}
McIndoe and the Guinea Pig Club
The First Transplants
In 1954, the first successful kidney transplant was carried out. It was between two twin brothers so they matched perfectly and the transplanted kidney was not rejected. In 1959, doctors discovered the drug imuran which could suppress the immune system and prevent transplanted kidneys being attacked by the patient’s immune system.
By 1967, the technology existed for the first successful heart transplant to take place. This was carried out by Christian Barnard. He was able to carry this out due to a number of factors:
He led a team of highly trained anaesthetists and nurses.
He used an electrocardiogram (ECG) machine to monitor the heart.
He used X‐rays to monitor the lungs.
Blood chemistry and urine were analysed in a laboratory.
{kind=link}
Christiaan Barnard
Surgery in the Present Day
Two significant advances which have been made in recent years are:
(i) Keyhole surgery – this is where a very small incision in the patient’s body is made and the surgeon uses fibre‐optic cables to look inside the body and an endoscope which has tiny tools for performing the operations. The advantage of keyhole surgery is that it does not leave a serious wound for the patient to recover from.
(ii) Micro surgery '‐' By magnifying the area a surgeon is working on it is now possible to perform operations on tiny nerves and blood vessels. For example, severed limbs or hands can be sewn back on and the feeling restored.